60 old male with right hemiplegia and right leg cellulitis
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.








This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
CASE: 60 years old male resident of nalgonda , agriculturer by occupation came to OPD with right side hemiplegia since 15 days and right foot swelling since 12 days.
HOPI:
Patient was apparently asymptomatic 15 days ago then he developed first weakness of Right upper and lower limb then pain and tingling sensation in the rt upper and lower limbs at night then he went to bed and slept, in morning he unable to move the right side of upper and lower limb, sensations also lost. History of slurring of speech and impairment of memory.They went to hospital there they diagnosed as rt side hemiplegia and gave the medication and advised to take the MRI scanning. So they came to our hospital.
Patient has history of injury to right big toe 12 days back followed by swelling of right dorsum and leg upto lower 1/3rd of leg , associated with low grade fever not associated with chills.
PAST HISTORY:
K/c/o diabetes mellitus and Hypertension since 6 months.for which he is on medication.
No H/o TB, asthma,epilepsy.
DAILY ROUTINE:
He daily wakes up at 5am ,does his daily routine and eats breakfast at 8 am.Then he goes to field for work and has his lunch at 1 pm returns home by 6 pm and does his dinner at 8pm.and goes to sleep at 9 pm .
PERSONAL HISTORY:
Diet: Mixed
Appetite: Normal
Bowel and bladder: Regular
Sleep:Adequate
Addictions: Occasional alcoholic since 35 yrs.
Smoking since 33yrs onwards.(occasion bidi for 30yrs,from 3 yrs onward regular 1 pack of bidi. Since 6 mns reduced to 2-3 per day ).
FAMILY HISTORY:
No significant family history
GENERAL EXAMINATION:
Patient is conscious,coherent and co-operative.well oriented to time,place and person.
Moderatly build and moderatly nourished.
No pallor, icterus, cynosis,clubbing, lymphadenopathy ,edema
Vitals:
BP:140/90(lft arm)
PULSE RATE:82/min
RESPIRATORY RATE:20cycles/min
TEMPARATURE:afebrile
* CNS EXAMINATION:
Right handed person
HIGHER MENTAL FUNCTION
Counsious ,oreinted to time place person
Speech normal
Behaviour normal
Memory intact
Intelligence normal
CRANIAL NERVE EXAMINATION
-OLFACTORY-normal
- optic : normal visual field
-oculomotor,trochlear,abducens -inract
-Facial nerve - right sided deviation of mouth
- vestibulocochlear- intact
- glossopharyngeal -intact
- vagus-intact
-accesory spinal ganglion nerve intact
- hypoglossal intact
Sensory system:
-fine touch: intact
-pain: normal
-temperature - normal
- vibration -normal
-stereognosis- normal
-two point discrimination-present
Motor system examination
Nutrition -
U/L. R. L
Normal. Normal
L/L. Normal. Normal
TONE:
U/L. R. L.
Normotania. Narmotonia
L/L
Normotonia. Normotonia
POWER. :- RIGHT. LEFT.
SHOULDER
flexion : 5/5 5/5
Extension 5/5. 5/5
Abduction 5/5. 5/5
Adduction 5/5. 5/5
Internal rotation 5/5. 5/5
External rotation 5/5. 5/5
Elbow:5/5. 5/5
Flexion. 5/5. 5/5
Extension:5/5. 5/5
Wrist:5/5. 5/5
Flexion:5/5. 5/5
Extension:5/5. 5/5
Abduction : 5/5. 5/5
adduction:5/5. 5/5
Hip
Flexion:5/5. 5/5
Extension. 5/5. 5/5
Abduction:5/5. 5/5
Adduction 5/5. 5/5
Internal rotation:5/5. 5/5
External rotation. 5/5. 5/5
Knee 5/5. 5/5
Flexion 5/5. 5/5
Extension. 5/5. 5/5
Ankle. 5/5. 5/5
Plantarflexion:. 5 /5. 5/5
Dorsiflexion. 5/5. 5/5
Toe. 5/5 5/5
Movements:5/5
REFLEXES:
-Corneal present
-Conjunctival present
-Abdominal: present
-Plantar: present
*DEEP REFLEXES:
Rt. Lt
Biceps : +++. ++
Triceps ++. ++
Knee : +++. ++
Ankle: +. +
**https://youtube.com/shorts/MUaK9YtwNSg?feature=share
**https://youtu.be/t05V0WYoQOc
*CEREBELLAR
-NYSTAGMUS absent
-DYSADEADOCHOKINESIA absent
**https://youtu.be/QXe7g7NEbDM
-FINGER NOSE tip- normal
Rhomberg sign -normal
Heel to knee intact
Meningial sign :
Kernigs sign negative
Brudzinski sign negetive
Cvs- s1 s2 heard ,no murmur,apex beat at mid clavicular line at 5 th intercoastal space.
Respiratory system
I: Chest bilaterally symmetrical, all quadrants
moves equally with respiration
P: Trachea central, chest expansion normal
P: Resonant
A: B/l equal air entry
B/I VBS
no added sound
Per. Abdominal examination :-
I normal
P soft non tender
No organomegaly
PROVISIONAL DIAGNOSES:
Right sided hemiplegia With right facial palsy (UML)- RECOVERED
And right leg cellulitis.
INVESTIGATIONS:
27/12/2022

USG:
28/12/2022:
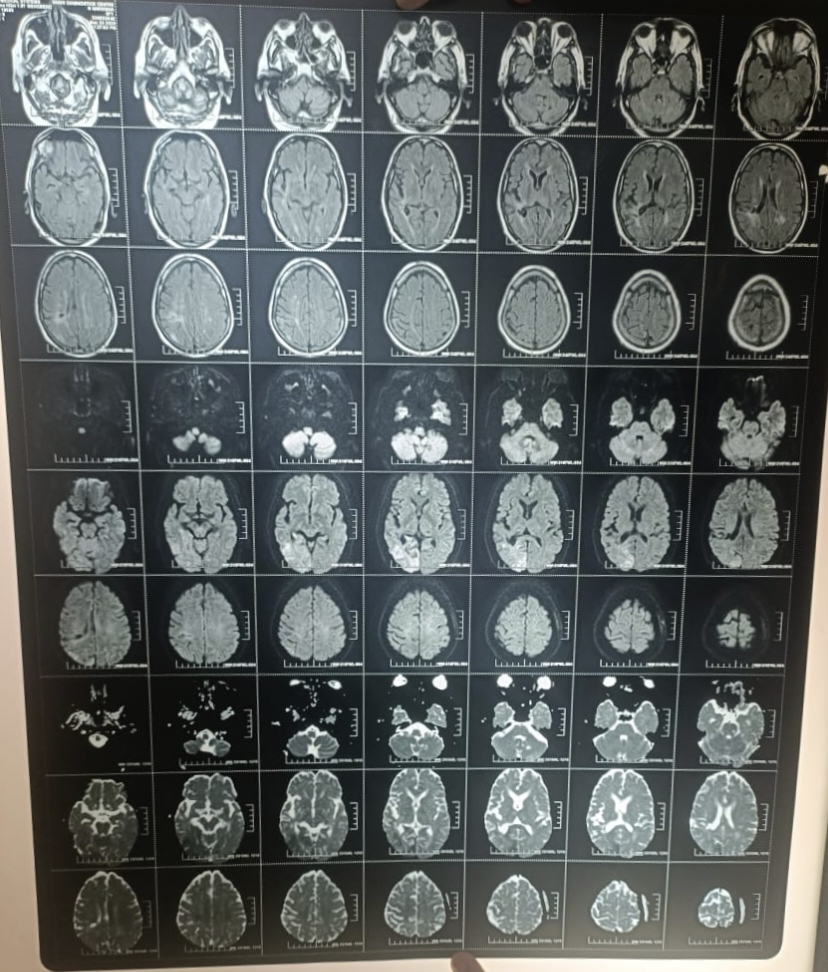
MRI:
Acute infart in left superior parietal lobe,pre central gyri,pre motor area,superior frontal gyrus,corona radiata and periventricular white matter embolic in nature.
FINAL DIAGNOSIS:
Right side hemiplegia with facial palsy due to acute ischemic stroke. Now he his RECOVERED
Right leg cellulitis.
Treatment:
T.Augmentin 625 mg PO/BD
T.Metrogyl:400 mg/PO/TID
T.Ecosprin AV 75/40/PO/night time daily
T.Glimi M1 BD
T.Neuroben forte once daily for 1 wk
T.Chymeral forte thrice daily for one wk
Regular dressing of lower limb
Right lower limb elevation.


Comments
Post a Comment